
FAQ on Intellectual Disability
- What is Intellectual Disability (ID)? [+]Intellectual Disability (ID) is a debilitating condition with deficits in cognitive functioning (IQ < 70) and adaptive skills. Developmental delay (DD) is the term used in children < 5 years, who show deficits in two or more developmental domains.
ID is often associated with behavioural problems (such as hyperactivity, autism, aggressive and self injurious behaviour), epilepsy and other neurological disabilities, resulting in a considerable psychological, social and economic burden to patients and families.
A full definition of ID, by the American Association on Intellectual and Developmental Disabilities (AAIDD), can be found by clicking this link. - How frequent is ID and what are the causes? [+]Intellectual Disability affects 2 - 3% of children and adults worldwide.
Causes of ID are many. Therefore, to identify the origin of ID in a child can pose a huge challenge to doctors. Causes of ID may occur as early as in fetal life or any time later in life. Examples include noxious hits to the fetal brain due to alcohol (fetal alcohol syndrome) or infections during pregnancy or later in life. Apart from such environmental and acquired causes, genetic origin is an important cause of ID.
Genetic causes by themselves are manifold and complex. Therefore many different tests are performed and many specialists are involved to elucidate those genetic causes.
Current guidelines for assessment of genetic ID are based on frequencies of single conditions and on the yield of diagnostic methods and procedures. Therefore cytogenetic techniques, such as karyotyping and array-CGH, which yield a causal diagnosis in 20% of cases, are considered priority. Despite high frequency and high diagnostic yield, no causal treatment is available for most of the conditions identified by these investigations. - What are treatable causes of Intellectual Disability? [+]Inborn errors of metabolism (IEMs) constitute a subgroup of genetic ID accounting for 2.5% of diagnoses. It is this subgroup, however, that does include conditions, which are causally treatable.
Despite the option to profoundly improve prognosis by implementing causal therapy, screening for IEMs is not performed systematically. This is explained by the fact that treatable IEMS are very rare and one wants to look at frequent conditions first. Another reason is the fact that there are no universal protocols summarizing comprehensively all IEMs causing treatable IDs. Furthermore there are no protocols indicating the type and order of tests to perform to make sure not to miss any of those conditions. - How many treatable IDs are there? [+]The number of treatable IDs is increasing. During the past two decades, an increasing number of IEMs have become amenable to treatments, and technologies for better recognition have been introduced into clinical and health care practice.
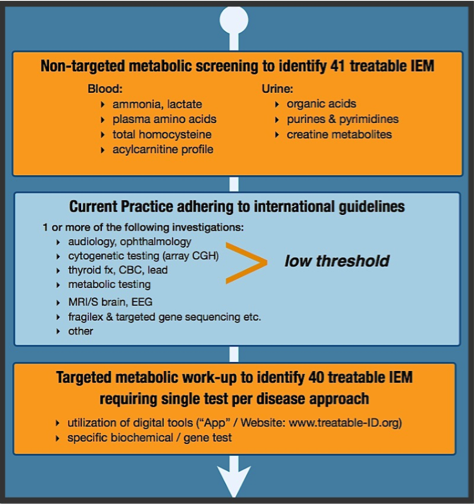
Therefore we undertook a systematic literature review to identify all treatable IEMs with Intellectual Disability as a prominent feature and to characterize types of treatments and evidence for effect. We identified as many as such 81 ‘treatable intellectual disabilities’. The review has been (tentatively) accepted for publication in the peer-reviewed journal Molecular Genetics and Metabolism. - How to diagnose treatable ID? [+]>50% of all disorders are potentially identified by routine metabolic screening tests in urine and blood. These group tests are easily available, relatively cheap and have the potential to identify 2 or more diseases. The test include serum acylcarnitine profile, plasma amino-acids, total homocysteine & urine organic acids, creatine metabolites, purines/pyrimidines.
If other tests in urine such as glycosaminoglycans and oligosaccharides are added to this routine metabolic screening, then 60% of all diseases can be identified. Such mucopolysaccharodises and oligosaccharidosis can often be recognized based on clinical features and thus do not (always) require routine screening.
For the remaining disorders a ‘single test for single disease approach’ is necessary. Because tests to diagnose these disorders are not widely available, and / or expensive, they cannot be done for everyone, but only after specific hints have become available through an extensive clinical by an experienced specialist. This APP supports the clinician in directing the differential diagnosis and plan for testing - What are the treatments and their (side-)effects? [+]We identified 91 treatments varying from sick day management, dietary modifications, supplements / cofactors, substrate inhibitors, stemcell transplant and gene therapy. The quality evidence varied from level 1-2 (20%) to 4-5 (60%); therapies with limited evidence can be very effective however, especially if started early in life (creatine substitution in AGAT deficiency for example). The majority of therapies with low levels of evidence are regarded as Standard of Care. Finally, most therapies on our list are accessible, affordable (Miglustat only expensive drug) and with acceptable side-effects.
A new Diagnostic Approach to ID
- Why a new approach? Because Time = Brain [+]The low frequency of these diseases should not prohibit an active process of identification. If we find more patients with treatable ID, we can improve their outcomes in many ways. In some, particularly young children treatment can halt progression of an otherwise ongoing developmental delay and preserve brain function. Other children may benefit because additional behavioural problems or epilepsy may improve on treatment. Even in the absence of causal therapy, determination of the genetic aetiology of ID is pivotal in generating and translating knowledge relevant to the anticipatory healthcare needs of the individual and their family –including genetic counselling- and minimizing gaps or disparities in care.
- What is the new protocol that facilitates the new approach? [+]The results of our systematic review prompted us to develop a protocol which acknowledges treatable ID as a priority and can be used by every single physician as an aid to evaluate a child with developmental delay and ID. The premise of this protocol is to consider treatability at first place, to provide state of the art evaluation for non-treatable conditions at the same time, and ultimately to give room for integration of new diagnostic technologies as they become available for clinical application. This protocol received attention at international conferences and benefits from global collaboration. It is being implemented as of September 2011 in BC Children's Hospital, Vancouver, Canada as part of the TIDE BC project.
Enrolling a large number of patients into our study with collection of data and tissues (DNA/urine) will allow us to evaluate the usefulness of the protocol (compared to previous practice) as well set the stage for innovative and comprehensive research on etiology and treatment of ID. - View the new TIDE Diagnostic Protocol [+]
Other FAQ (on the functionality of this tool)
- How does the tool work? [+]Please visit our 'Help' section. Here you'll find a detailed description of the different features in this tool.
- I miss some 'Signs & Symptoms" that are not listed with a particular disease, while I think they should be listed [+]For each disease only the most characteristic, specific and consistent features are listed here.
We emphasize that that absence or presence of specific signs and / or symptoms not fitting our list does not in any way rule out the specific disorder in a patient. Also, these data are subject to change as new diagnostic techniques provide novel insights into the spectrum of phenotypic presentation and natural history of metabolic diseases. This tool will be updated accordingly at regular intervals. - I used the search function but the diseases the search engine returned do not list the signs & symptoms I entered? [+]Please note that for each disease only the most characteristic, specific and consistent features are listed. On the disease page you will also find general information on the disease (via the "Disease Info" button). In this section other signs & symptoms might be mentioned that didn't meet the criteria for our list. Since the search engine crawls all information on the disease pages it incorporates that information as well.
We emphasize that that absence or presence of specific signs and / or symptoms not fitting our list does not in any way rule out the specific disorder in a patient. - What tests are defined as "Routine metabolic screening tests"? [+]Serum acylcarnitine profile, plasma amino-acids, total homocysteine & urine organic acids, creatine metabolites, purines/pyrimidines.
- For epilepsy and behavioral / psychiatric symptoms, there is lack of detail in the clinical description [+]Due to limited literature data, it is currently not possible to provide more detail on the behavioural or psychiatric disturbances in these rare conditions.
- Using my iPad / iPhone, some of the links in the literature section of the disease pages don't seem to work [+]This is a known issue and affects people using iOS5. Unfortunately the search strings that are used to crawl the PubMed website are not supported by iOS5. This will be fixed once the iOS app is launched. Until that time, those links are available if you access the tool via your regular computer.